

The hair/thread tourniquet syndrome is a clinical phenomenon characterized by hair, thread or similar material tightly wrapping around an appendage such as digits or genitalia, leading to circumferential constriction, edema and eventual ischemia. They can even occur on the taste buds as noted in this case report! Due to the risk of strangulation and necrosis, it is an important differential diagnosis for the inconsolable infant.

From Wikimedia commons – 2016
The median ages for finger, toe and external genitalia involvement were found to be three weeks, four months, and two years, respectively per Barton, et al [1988]. Human hair was the cause of constriction in 79% of children with toe involvement; this was linked to maternal telogen effluvium experienced by approximately 90% of mothers during the postpartum period [an association reinforced by Strahlman, 2003]. Synthetic fiber or thread was the cause of strangulation in 88% of children with finger involvement, and likely related to use of mittens. Most cases among children with constriction to external genitalia involve circumcised boys, and materials implicated extend to rubber bands and other elastic items.
Unwind or incise has been the standard of treatment; and the approach selected depends on damage to appendage and depth of constricting fiber or hair.
When the constrictor is superficially embedded, less invasive approaches are recommended:
- Grasp the free end of hair or thread firmly with gloved finger or preferably fine forceps or hemostat; and gently unwind from the appendage.
- Blunt probe method: Gently insert blunt probe or metal earwax curette between skin and hair [may be more accessible on dorsal aspect]; and cut fiber with fine-tipped scissors or scalpel blade directed against the surface of probe or curette.
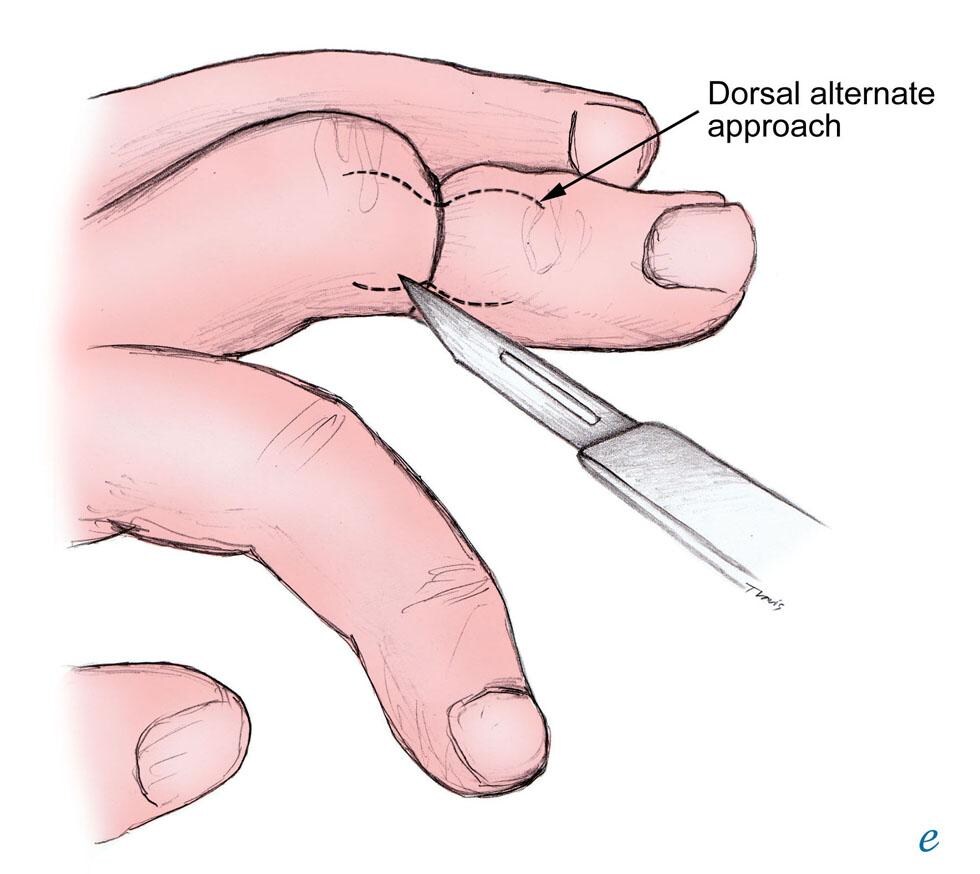
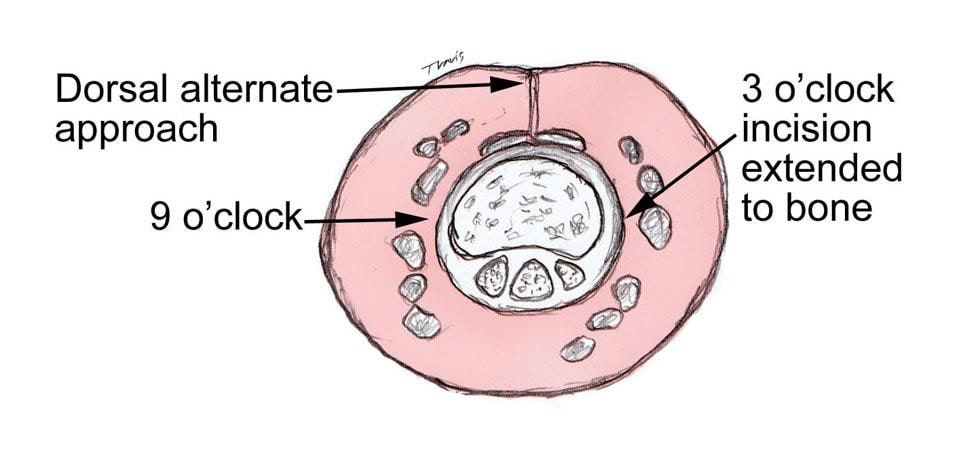
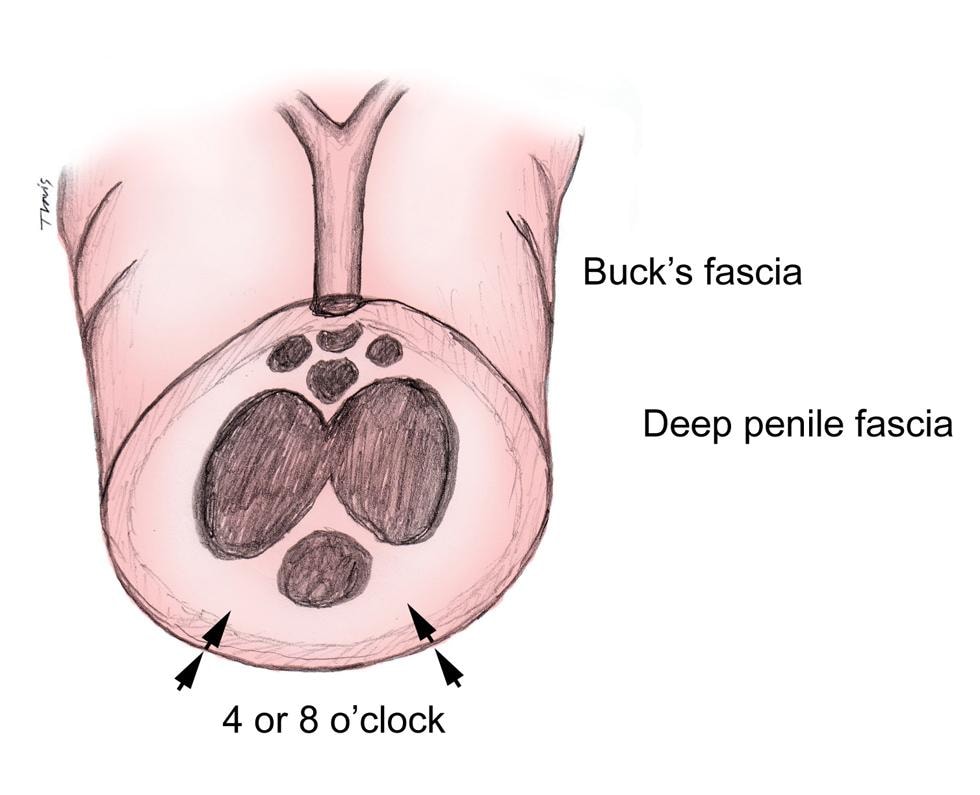
In more severe cases where there is significant edema or fiber has penetrated soft tissue, the incisional approach is required. Site of incision is selected to avoid underlying neurovascular bundles. For digits, an incision is made longitudinally at 3-o’clock or 9-o’clock position, with blade perpendicular to strand and skin surface, in proximal to distal direction and to depth of bone to ensure constricting fiber is cut completely. The alternative is an incision at the 12-o’clock position, the dorsal surface of the digit and parallel to the extensor tendon. For the penis, incision is made at lateral inferior aspect, 4-o’clock and 8-o’clock positions.
O’Gorman and Ratnapalan [2011] published the first case report describing removal of hair tourniquet using depilatory cream as other methods were found to be difficult especially with swollen appendage.
Over the counter depilatory creams such as NairTM are thioglycolate-based, and work by disrupting the chemical bonds of hair keratin. Therefore, this is limited to hair tourniquets and unfortunately will not work in cases with other fiber or thread constrictions. The cream is applied to the region of hair tourniquet with subsequent wait time of approximately 3-10 minutes to allow complete hair breakage. Subsequently, thoroughly remove and wash with water. This treatment should be avoided in cases with broken skin. Emerging case and anecdotal reports have highlighted this approach to be effective and painless, a simple procedure to treat hair tourniquet syndrome.
In cases where there is more significant inflammation and the hair tourniquet is deep/longstanding consider prescribing an oral antibiotic. Cephalexin, Amoxicillin/clavulanate and Clindamycin are among several reasonable choices.
References
- Alruwaili N, Alshehri HA, Halimeh B. Hair tourniquet syndrome: Successful management with a painless technique. International Journal of Pediatrics and Adolescent Medicine 2015;2:34-37
- Barton DJ, Sloan GM, Nichter LS, Reinisch JF. Hair-thread tourniquet syndrome. Pediatrics 1988;82[6]:925-928
- Claudet I, Pasian N, Marmchal C, Salanne S, Debuisson C, Groteau E. Hair-thread tourniquet syndrome. Arch Pediatr 2010;17:474-479
- Loiselle JM, Cronan K. Hair Tourniquet Removal. Textbook of Pediatric Emergency Procedures. Henretig FM, King C [Eds]. Philadelphia, PA: Lippincott Williams & Wilkins 2008:1065-1068
- O’Gorman A, Ratnapalan S. Hair tourniquet management. Pediatr Emerg Care 2011;27[3]:203-204
- Peckler B, Hsu CK. Tourniquet syndrome: a review of constricting band removal. J Emerg Med 2001;20[3]: 253-262
- Strahlman RS. Toe tourniquet syndrome in association with maternal hair loss. Pediatrics 2003;111[3]:169-170










{kind=link}
{kind=link}
{kind=link}