

According to the AAP’s 2006 Clinical Practice Guideline, bronchiolitis is the most common lower respiratory tract infection (LRTI) in infants and is caused by a virus – most often RSV in 70-80%, Human metapneumovirus in 10-20%, and then assorted rogues such as Adenovirus, Rhinovirus, Parainfluenza, and Influenza pulling up the rear. Its cardinal pathophysiologic features include;
- Acute inflammation
- Edema and necrosis of epithelial cells lining small airways
- Increased mucous production
- Bronchospasm
It is rare in the first month of life, and peaks between ages 2-5 months – with 90% of children having some sort of RSV infection in the first 2 years of life. Most cases are seen between December and March. The symptoms include those of both upper and lower respiratory tract infections.
URI Symptoms
- Rhinitis[/list]
LRTI Symptoms
- Tachypnea
- Cough
- Wheezing
- Crackles
- Accessory muscle use
- Nasal flaring
- Fever in only 30%
[/list]
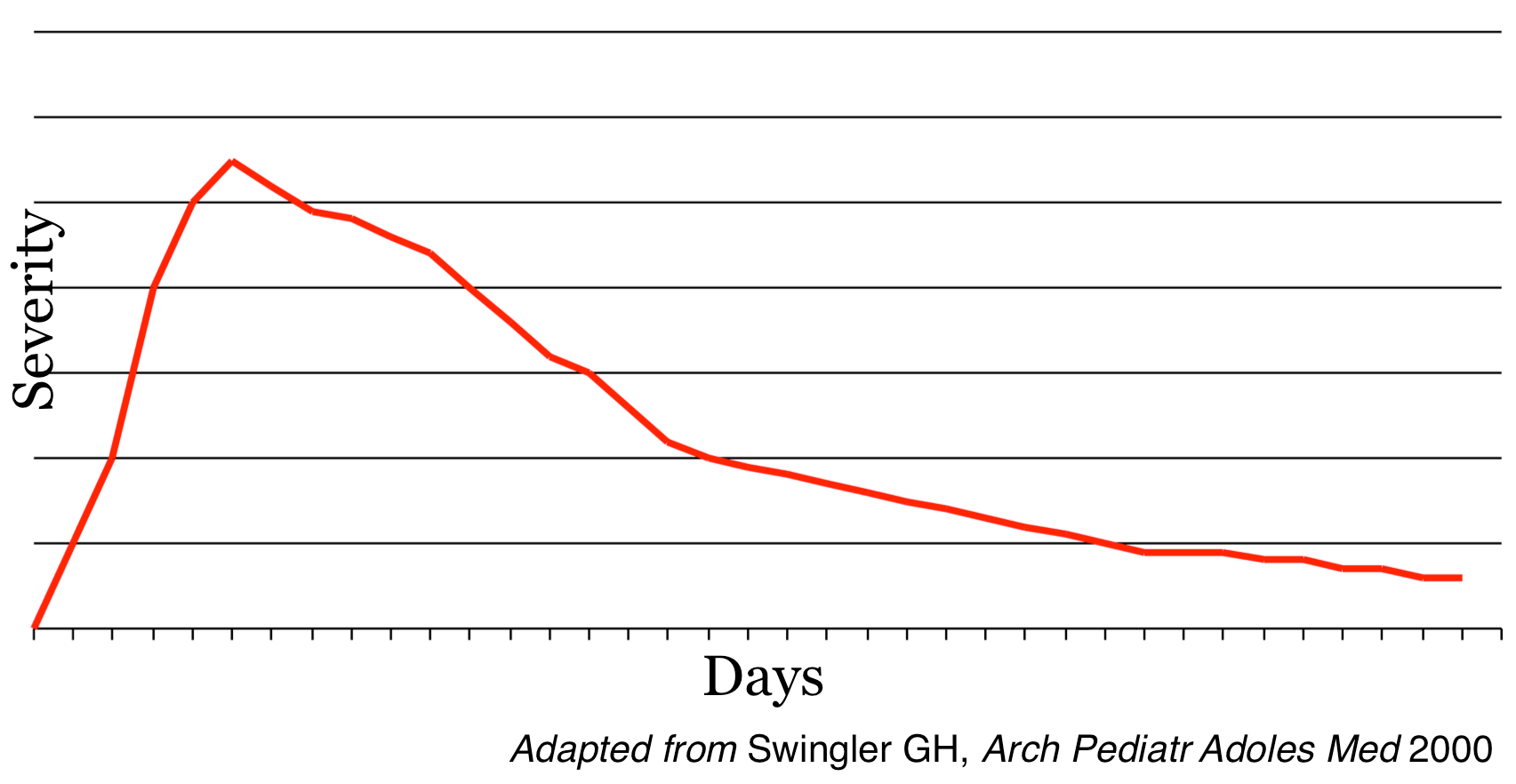
In general the clinical severity of symptoms peak between the 4th through the 6th day. Though Human metapneumovirus may see a later peak than RSV by a day or two.
The annual cost of hospitalizations is estimated at $700 million dollars.
Interestingly the rate of inpatient stays has increased since the development of pulse oximetry – Hmmm .
Stay tuned to this site for a series of posts exploring various diagnostic and therapeutic options for bronchiolitis – In total I hope that this will be a ‘mini-elective’ in managing this persistent illness.
Special thanks to my colleague, and local bronchiolitis aficionado Todd Florin, MD, MSCE.










[…] you haven’t checked out Part 1 of the Bronchiolitis series do so here – otherwise, let us trudge onward. This time, towards a potential therapy that is used in […]
[…] to part 3 of the bronchiolitis series. Parts 1 and 2 are here and here. We’ve a;ready explored how (un)helpful albuterol can be, so what about other […]
[…] I, II, and III are still there for those of you yet to dive in but now we turn our attention to a […]
[…] you haven’t read parts I, II, III, IV or V what are you waiting for? Today’s post will focus on testing in […]
[…] seemingly endless spew of bronchiolitis related content here on the PEM Blog. Check out editions I, II, III, IV, V, and VI if you’d like. Today we’ll be focusing on additional modes […]
[…] this is the final post in the bronchiolitis series. I hope you’ve enjoyed it. Parts I, II, III, IV, V, VI, and VII aren’t going anywhere – so check them out if you […]
[…] I: Let’s just get our definitions straight all right? […]