
Most of the readers of this blog will have diagnosed at least one case of otitis media. If you haven’t then you’re not working enough (kidding). You may also have had discussions with parents of children presenting with ear pain (usually at 2AM) about how their child’s TM doesn’t look like an ear infection right now and that it could look like one in a day or two, and that PMD follow up is appropriate. This often results in a quizzical look from mom, an awkward silence, and then a request for a prescription for antibiotics. Perhaps you are a stalwart clinician (hopefully you are) and you stand your ground, refusing to relent to antibiotic pressure – citing your examination and the available literature as reasons why you don’t need to prescribe amoxicillin right now. Maybe things go well, you treat the otalgia (PLEASE treat the pain!) and everyone goes home without a tantrum (you included). Maybe, a new otitis media guideline/position statement just came out from the AAP that will make these scenarios more common in the ED. This my readers is why I’ve written this post.
The big take home point is that A LOT of otitis media is viral.
What does the AAP Say?
In the recently published The Diagnosis and Management of Acute Otitis Media the authors recommend the following regarding the diagnosis and treatment of uncomplicated AOM in children 6 months to 12 years:
Diagnose otitis media when…
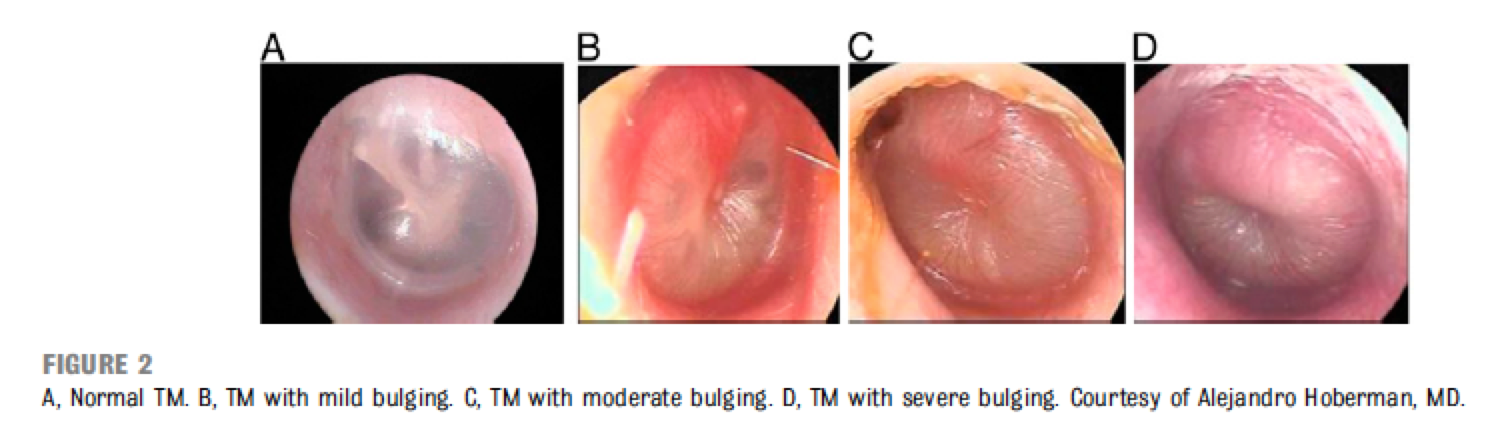
The TM has moderate to severe bulging and/or new onset otorrhea in the absence of otitis externa
You could also diagnose AOM (though the level of evidence is less clear than the above) if…
Children present with mild bulging of the TM AND recent (less than 48 hours) onset of ear pain (holding, tugging, rubbing of the ear in a nonverbal child) or intense erythema of the TM
You should NOT diagnose AOM if…
The TM does not have an effusion
The treatment of AOM should include…
Pain management (NSAIDs or topicals like Auralgan (if available) because antibiotic therapy of AOM does not provide symptomatic relief in the first 24 hours and even after 3 to 7 days, there may be persistent pain, fever, or both in 30% of children younger than 2 years.
You should almost always treat…
Severe: Moderate or severe otalgia or otalgia for at least 48 hours or temperature 39°C Nonsevere bilateral AOM in young children: The clinician should prescribe antibiotic therapy for bilateral AOM in children 6 months through 23 months of age without severe signs or symptoms (ie, mild otalgia for less than 48 hours and temperature less than 39°C [102.2°F]) You can either treat or offer observation with PMD follow up if the child worsens or fails to improve in 48 to 72 hours for… Nonsevere unilateral AOM in young children: unilateral AOM in children 6 months to 23 months of age without severe signs or symptoms (ie, mild otalgia for less than 48 hours and temperature less than 39°C [102.2°F]) Nonsevere AOM in older children: Unilateral AOM in children 24 months or older without severe signs or symptoms (ie, mild otalgia for less than 48 hours and temperature less than 39°C [102.2°F]) You should generally treat AOM with… High dose (80mg/kg divided bid) Amoxicillin as your first choice You probably shouldn’t use Amoxicillin and instead give Augmentin if… The patient has received amox in the past 30 days The patient has concurrent purulent conjunctivitis (non-typeable H. flu is the likely pathogen and the combo infection will respond better with a beta lactamase inhibitor) The patient has a history of treatment failure with Amoxicillin You should not… Offer prophylactic antibiotics to prevent recurrent AOM (no matter how much the parents beg for them) You can refer to ENT or at least bring up the idea of tympanostomy tubes if… The child has recurrent AOM (3 episodes in 6 months or 4 episodes in 1 year with 1 episode in the preceding 6 months) You should make sure that… Your patients have been getting their pneumococcal conjugate and influenza vaccines It’s going to be a lot easier to withhold antibiotics in a primary care office than in the ED at 2AM. I certainly advocate for adhering to the best current evidence, and in order to do this here is what I recommend. Sure. Note that at least 87% of Streptococcus pneumoniae isolates (the #1 AOM pabacterial pathogen) are susceptible to high dose Amox. So that should be your first choice. Check out this table for additional options for initial therapy. Here are some pics of tympanic membranes so you don’t have to Google themHow does this affect my practice?
Could you summarize what antibiotics are OK for AOM?

Bonus!










very helpful
Thank you