

COVID-19 case numbers are soaring across the Unites States. There were early fears that SARS-Cov-2 would be joined by seasonal influenza viruses to create a double whammy and further overwhelm the healthcare system. Thus far, that hasn’t been the case. In this post I’ll share some information on why we suspect that we won’t be seeing as much flu as initially expected.
The 2019-20 flu season ended abruptly
Seasonal flu cases in the Northern Hemisphere usually start to peak in February and tail off by May. Flu season obviously begins in the prior fall. Interestingly, this year we noted that flu positive case numbers dropped off significantly in April. See the figure below from Nature.

Why was this the case? No single reason accounts for the drop off – Fewer people may have sought care and testing in the early parts of the pandemic, and social distancing prevents illness spread broadly. In the first few pandemic months in the US positive flu tests decreased by 98%; tests decreased by ~60% per Olsen et al. from MMWR. The flu season was ultimately rated “moderate” by the CDC anyway – so a little lower than recent years but not dramatically so.
Social distancing, masks, and hand washing prevent more than just COVID-19
‘Nuff said…
The flu largely skipped South America this year
Between April and July 2020 there were very few influenza cases in the Southern Hemisphere. Per data from the MMWR there were 51 total cases of influenza in approximately 83,000 tests sent in Australia, Chile, and South Africa! The flu is less transmissible than SARS-Cov-2 and despite some poor control of COVID-19 in some South American nations they still didn’t see much influenza. Limiting international travel certainly played a role. Recall that flu moves around the globe following the winter season largely. Fewer people,e moving around probably lead to fewer cases.
More people got flu shots (at least in some places)
Some countries at least saw increased flu vaccination rates year over year – Australia for instance noted year over year gains in the number of flu shots administered – 7.3 million by May 2020, 4.5 million in 2019, and 3.5 million in 2018. Public health campaigns likely played a role in these increases.
The intangibles – And what about other viruses?
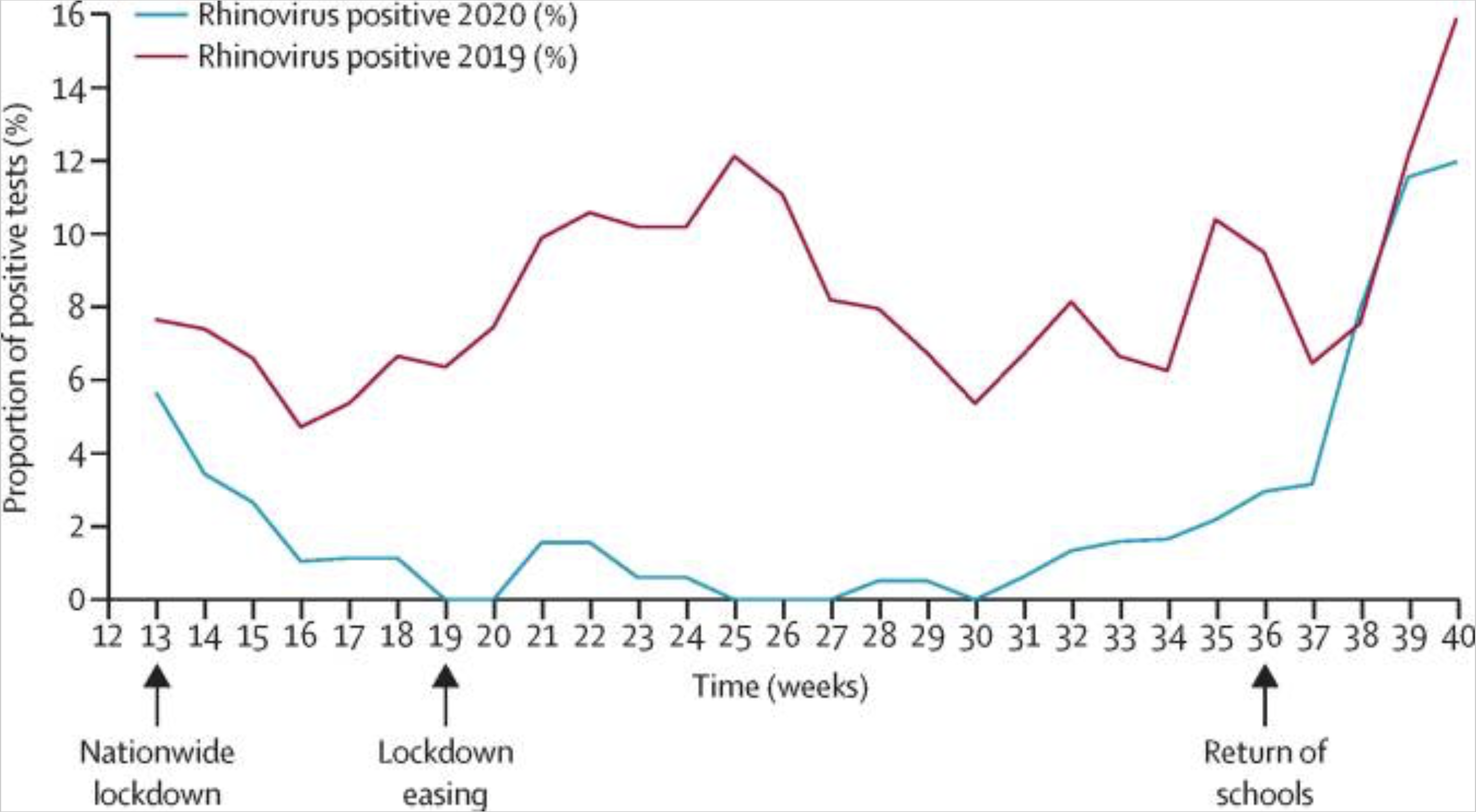
There is still a lot we don’t know about influenza and how it spreads year to year. Having a mild flu season this year might make it harder to predict which strains will predominate in future years. And these trends are not just about influenza, RSV levels have been surprisingly low as well. On a personal level I’m not seeing nearly as much bronchiolitis as in years past. However rhinovirus activity, especially in certain regions, has remained relatively high. Per Poole et al. a surge in rhinovirus was noted post-lockdown when in person schooling resumed in Southampton, UK. They concluded that children were a large reservoir for rhinovirus – which has dozens of strains that circulate and cause the common cold. Rhinovirus may be more hardy on surfaces than other viruses. But nobody is exactly sure why there have been regional disease prevalence spikes. And finally, some researchers wonder if rhinovirus outbreaks mitigated the impact of the H1N1 pandemic back in 2009-10. Could this have the same effect on SARS-CoV-2? Time will tell.
References
Olsen, S. J. et al. MMWR Morb. Mortal. Wkly Rep. 69, 1305–1309, 2020.
Chan, K. H. et al. Monitoring respiratory infections in covid-19 epidemics. Br. Med. J, 2020.
Poole et al. Physical distancing in schools for SARS-CoV-2 and the resurgence of rhinovirus. Lancet Respir Med. 2020 Dec; 8(12): e92–e93.
Jones, How COVID-19 is changing the cold and flu season. Nature, 2020.
Jones, How coronavirus lockdowns stopped flu in its tracks. Nature, 2020.
Wu, A., Mihaylova, V. T., Landry, M. L. & Foxman, E. F. Interference between rhinovirus and influenza A virus: a clinical data analysis and experimental infection study. Lancet Microbe 1, e254–e262 (2020).










Your point of view is very good. Totally agreed