
In conjunction with Taming The SRU and the University of Cincinnati Department of Emergency Medicine’s Annals of B Pod I am proud to present this article on pediatric supraventricular tachycardia (SVT) – our first of many collaborations. The case discussion was authored by PGY3 Resident Tyler Winders, MD. Fourth year UC EM Resident Benjamin Ostro, MD headed the charge. And not shockingly, the input of Dr. Christopher J. Statile, Assistant Professor in Pediatric Cardiology at Cincinnati Children’s Hospital Medical Center, and Dr. Peace Chike Madueme, Assistant Professor in Pediatric Cardiology at Cincinnati Children’s Hospital Medical Center was heart-stompingly valuable. So without further conduction delay we discuss the management of pediatric, and especially neonatal supraventricular tachycardia.
Case Presentation
The patient is a healthy 3 week old male with no past medical history. He was born full term via uncomplicated Cesarean Section who presents with increased fussiness. His mother states the patient has simply not been acting like himself. He was taken home on hospital day 1 without issues, but in the last 24 hours, he has been quite fussy. His mother became concerned when he was unable to take his bottle today. The child has been refusing to eat and has been increasingly difficult to console. He has also had less wet diapers than normal today. Mom has not noticed cyanosis during feeding, recent illnesses or fevers. She also denies the presence of emesis, diarrhea, rashes, congestion, or cough.
Physical Exam
Vital Signs: T 98.6 HR 275 RR 30 BP 95/54 O2 Sat 100%
General: crying on infant warmer, fussy
HEENT: normocephalic, atraumatic, soft anterior fontanelle
Cardiac: tachycardic but regular, no m/r/g, no JVD, strong central pulses
Pulmonary: symmetric chest rise without accessory muscle use, no stridor, CTAB
Abdominal: soft, non-distended, no organomegaly
Skin: normal turgor, capillary refill <3 seconds
Extremities: warm and well-perfused, no acrocyanosis
Hospital Course
The patient presented with a heart rate of 275 but was warm and well perfused with strong central pulses and brisk capillary refill. EKG was obtained and consistent with supraventricular tachycardia (SVT).
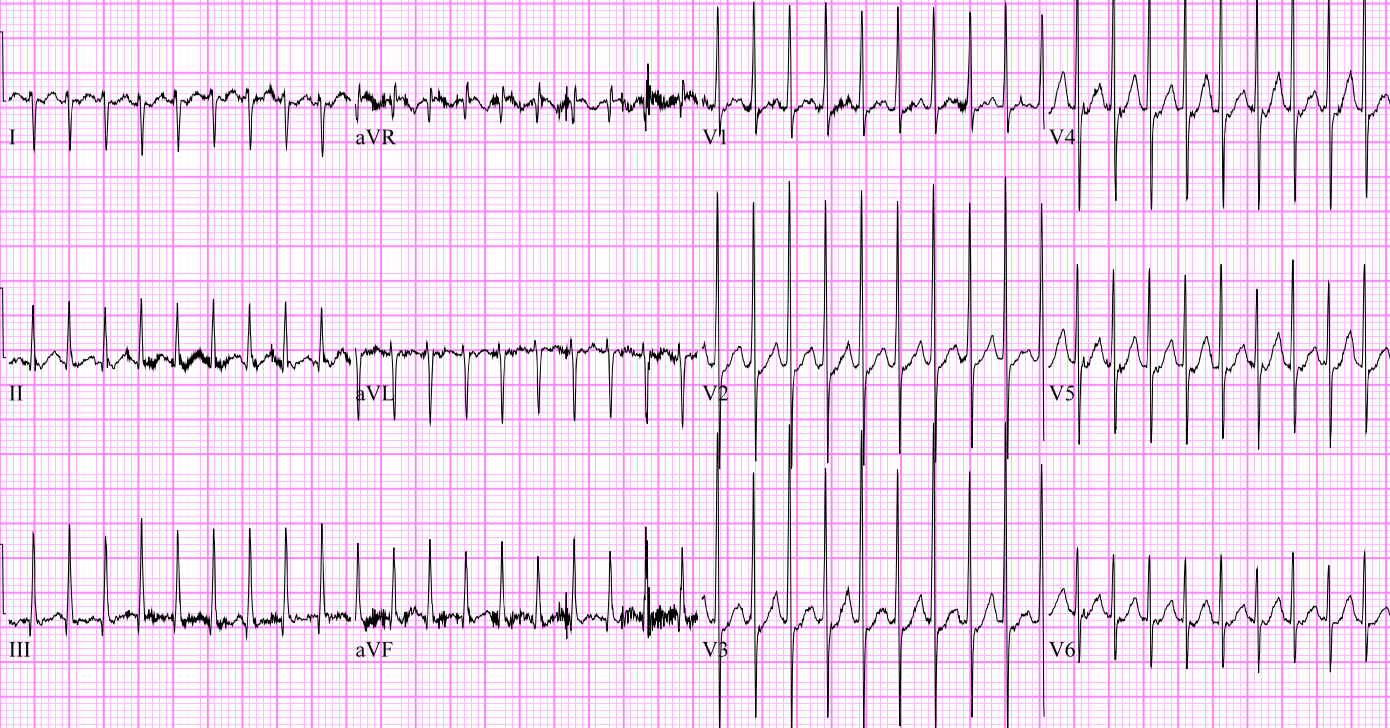
The EKG shows a narrow, regular complex tachycardia consistent with SVT
Pedi-pads were placed just in case the patiet decompensated and became unstable. However, the patient remained hemodynamically stable therefore vagal maneuvers were attempted first, and the patient converted to normal sinus rhythm within 5 seconds of ice application to his face. He ate well and was back to his baseline mental status soon after his cardioversion. The patient was admitted to cardiology where echocardiogram was performed and was unremarkable. The patient remained in normal sinus rhythm throughout his hospital stay. The patient will follow up with cardiology as outpatient and was not sent home on any anti-arrhythmics.
Approach to SVT in Neonates
Supraventricular tachycardia is the most common arrhythmia in children. SVT most often affects children with normal hearts, although structural abnormalities and critical illness are considered risk factors. The two most common mechanisms of SVT are atrioventricular reentrant tachycardia (AVRT) and atrioventricular nodal reentrant tachycardia (AVNRT). One electrophysiology study of 139 patients found AVRT to account for 73% of cases and AVRT to account for 13% of cases.
With patients presenting in SVT, it is important to begin with the basic PALS algorithms and immediately differentiate stable versus unstable. If the patient is unstable, simply remember 2 joules per kilogram synced cardioversion, but if the patient is stable, recognize there are multiple treatment options available. As far as recognizing the unstable infant, look for evidence of heart failure, significant pallor, or decreased level of consciousness in addition to simply checking a blood pressure. If the patient requires cardioversion, PALS recommends 0.5-2.0 J/Kg delivered synchronously. Pediatric pads are preferred, but adult pads are an option if no pediatric pads are readily available.
Our patient fell into the stable, narrow-complex tachycardia algorithm. It is important to keep in mind that wide complex tachycardia often has significantly different underlying pathology than narrow complex and should be treated as such. The cutoff for a wide complex tachycardia in pediatrics is a QRS > 0.09 seconds. [4] Since our patient was in narrow complex tachycardia, we elected to trial vagal maneuvers prior to initiating pharmacologic interventions. The preferred vagal maneuver in infants is the diving reflex. The infant should be placed in a sitting position, and a bag of ice should be placed on the infant’s face while simultaneously laying the infant back quickly. A second option is rectal stimulation using a thermometer. The concept behind both is to elicit a strong vagal response in a patient unable to voluntarily valsalva. One retrospective study found vagal maneuvers to be successful in 63% of SVT in children. [3]
If vagal maneuvers fail, adenosine is considered the drug of choice as it is a short acting but quite powerful AV nodal blocking agent that interrupts the reentrant conduction pathways causing the arrhythmia. [4] The recommended dosage in pediatrics is 0.1 mg/kg. If this is not successful, providers may reattempt with 0.2 mg/kg (max of 6mg and 12mg respectively). Other medications to consider would be amiodarone (5mg/kg over 20-60 minutes) or procainamide (15mg/kg over 30-60 minutes), but both of these medications may cause hypotension and involvement of a pediatric cardiologist prior to initiation may be advisable.
Q&A With The Experts in Pediatric Cardiology at Cincinnati Children’s Hospital
If ice applied to the patient’s face does not work in the stable infant in SVT, have you had success with continued efforts at vagal maneuvers or do you move on to pharmacologic therapy?
I would continue to try vagal maneuvers while stable. Often, maneuvers are not done appropriately and others may work. After 15 min of being unsuccessful, medical therapy is appropriate but take into consideration how long the patient is perceived to have been in tachycardia (a person in tachycardia all day should be converted faster). -Dr. Christopher J. Statile and Dr. Chike Madueme
Discussing pharmacologic cardioversion. There is a decent amount of evidence for verapamil, but it seems like adenosine is the preferred drug in the ED. What is your experience, if any, with verapamil?
Verapamil is a higher class drug and warrants more experience than adenosine. We don’t use it much (except for our EP colleagues) and it has a longer half life. As such, we use it as a tertiary medication and would never use it in the ED on a stable patient. If the patient is stable and cannot be converted using adenosine in the ED we would recommend cardiology consultation and likely transfer to the cardiac ICU for further treatment. -Dr. Christopher J. Statile and Dr. Chike Madueme
Let’s say we’ve tried vagal maneuvers and adenosine without success and now are considering a third line agent such as amiodarone, procainamide, and digoxin. What is your preferred third-line agent for cardioversion in the stable neonate in svt once vagal maneuvers and adenosine have failed?
This question is not so straight forward. It depends on whether there has been transient response with resumption of tachycardia or no response at all. For the former, often times the circulating catecholamines need to be decreased (for example with a beta blocker or sedation) before a repeat attempt at rate control is made as that may be the reason for continuing to re-enter into tachycardia. For the latter, it may not be SVT after all. In either case, cardiology should be aware as this no longer qualifies as simple SVT. -Dr. Christopher J. Statile and Dr. Chike Madueme
At what point would you consider synchronized cardioversion for a stable neonate in SVT?
In the stable infant, this usually is not necessary if it is true SVT. We would rarely use synchronized cardioversion for a stable neonate in re-entrant SVT. However, if the infant was in atrial flutter, synchronized electrical cardioversion may be necessary. Again this should not be done without input and involvement of a cardiologist as long as the patient is stable. If the patient is unstable, then electrical cardioversion is indicated. -Dr. Christopher J. Statile and Dr. Chike Madueme
When is it appropriate to consult pediatric cardiology? Does every stable patient that undergoes successful cardioversion in the ED require inpatient cardiology consultation? Or are these patient’s safe for outpatient follow up?
All patients with SVT that are cardioverted should receive a consultation in the ED by the cardiology fellow. Whether the patient needs to be admitted and monitored in the hospital depends on the circumstances surrounding the SVT. If the patient is less than a year of age, most will be admitted for observation. Often these patients will be started on an anti-arrhythmic medication. At the very least the parents will have to undergo heart rate monitoring training. The reason for this is that it is often unclear how long the infant was having tachycardia. It is also often hard, if not impossible, to tell that they are in SVT without listening or taking a heart rate. These patients also deserve an echocardiogram at diagnosis for the same reason. It is often unclear how long the infant or toddler has been in tachycardia and while SVT is well tolerated for short periods of time up to a few hours, if in SVT for longer (multiple hours to days) they can develop marked ventricular dysfunction and can get quite sick. Older children that can convey that their heart is beating fast and can usually be discharged from the ED with cardiology follow up after a cardiologist has evaluated at the tracings and maybe even seen the kid in the ED. -Dr. Christopher J. Statile and Dr. Chike Madueme
What if you are in the community taking care of a child with svt and vagal maneuvers and adenosine have failed? Should the patient be transferred to the nearest children’s hospital with a cardiologist or is cardioversion an option if your more than 60 minutes away?
I would probably double the dose of adenosine and speak to a cardiologist. The reality is that if the rhythm is not converting with adenosine it’s probably not re-entrant SVT and likely flutter, congenital JET (junctional ectopic tachycardia), or PJRT (permanent junctional reciprocating tachycardia). I would still get in touch with a cardiologist and have them walk you though what to do next as long as the patient is stable. -Dr. Christopher J. Statile and Dr. Chike Madueme
References
- Colluci R, Silver M, et al. “Common Types of Supraventricular Tachycardia: Diagnosis and Management.” – American Family Physician. N.p., Oct. 2010. Web. 21 July 2015.
- Garson A, Gillette PC, Mcnamara DG. Supraventricular tachycardia in children: clinical features, response to treatment, and long-term follow-up in 217 patients. J Pediatr. 1981;98(6):875-82.
- Kugler JD, Danford DA. Management of infants, children, and adolescents with paroxysmal supraventricular tachycardia. J Pediatr. 1996;129(3):324-38.
- Spencer B, Chacko J, Sallee D. The 2010 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiac care: an overview of the changes to pediatric basic and advanced life support. Crit Care Nurs Clin North Am. 2011;23(2):303-10.









