
The Case
A 14 year old male was tackled while playing football and has pain along the angle of his jaw. He can open and close his mouth without pain. He does have pain to palpation along the body of the mandible adjacent to 2nd/3rd left inferior molars. There are no loose teeth and he feels that they are in normal alignment. He can bite down on a tongue depressor, and feels pain at same site when you flick the tongue depressor and it vibrates. He wants to know if he has a mandible fracture?

from learningradiology.com
Diagnosis
Fortunately his X-Rays were read as normal. Before moving on take a look at this representation of mandible anatomy.
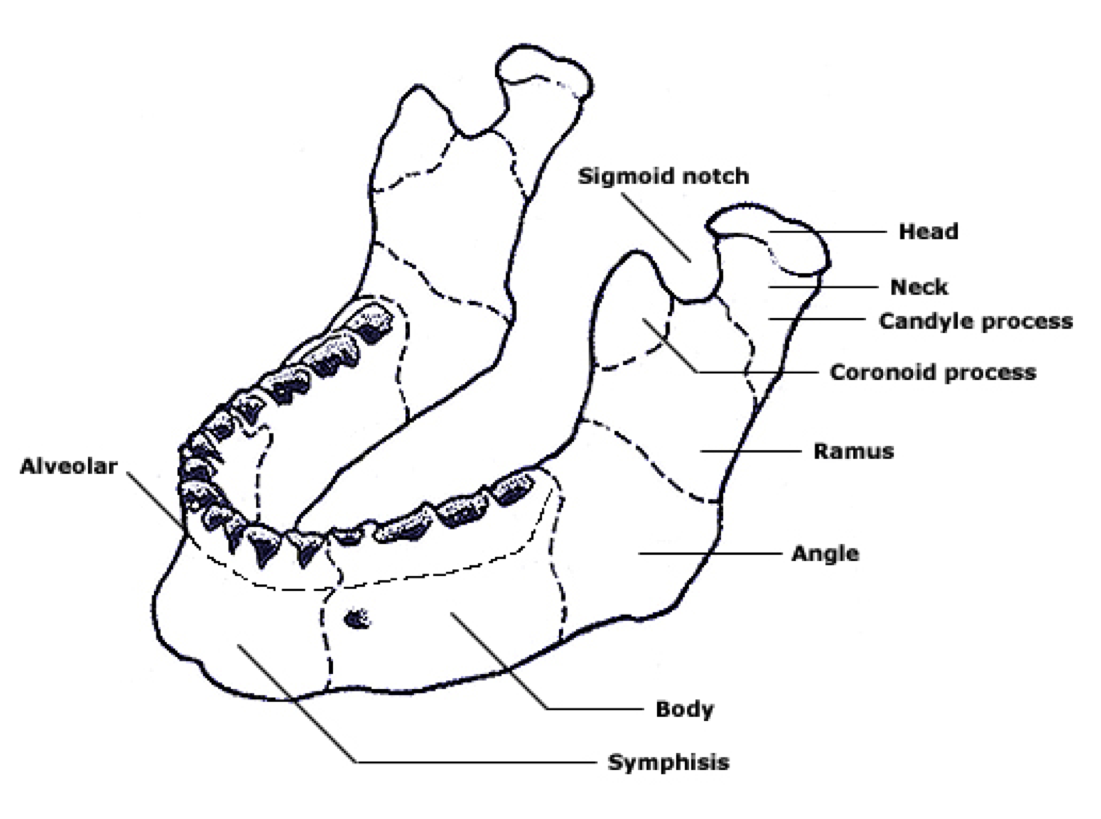
The jaw!
In the Pediatric ED the peak incidence 16-20 year. As you might expect males are 3:1. In patients less than <10 years old the condyles are the most common location, whereas in those >10 years old you see fractures of the symphysis, body, and/or ramus. Multiple fractures are seen in 40-60% – These are more common when patients are >13 years old. C spine injuries are also seen in <1% whereas dental injuries are much more common – 20-30%. Fractures of the condyle and symphysis are seen more often in falls and motor vehcile accidents, whereas assaults/blunt trauma lead to fractures of the body and angle. In adults the fracture breakdown by cause is:
- MVC 40%
- Assault 40%
- Fall 10%
- Sports 5%
- Other 5%
What exam findings can help diagnose a mandibular fracture?
- Tenderness over fracture site
- Malocclusion
- Bruising in floor of mouth
- Mucosal/gingival lacerations
- Chin deviation
- Pain when opening/closing mouth
- Inability to bite down on a tongue depressor
- Tooth fracture
- Lip numbness (inferior alveolar nerve injury)
Pro-Tip: Bleeding /lacerations along the alveolar ridge suggests an open mandibular fracture
Are chin lacerations associated with fractures of the mandible?
Management
Imaging
- Malocclusion
- Trismus
- Broken teeth
- Pain with mouth closed
- Step-off deformity
Though your mileage may vary – this study was done in adults, and I still advocate for X-Rays. However, if the patient does have one of the above findings, and has normal X-Rays and can eat and talk I don’t rush them to the CT scanner as they patient may have a non-operative non-displaced fracture that wouldn’t necessarily change management significantly.

Fracture of the body of the mandible
Treatment
Prognosis
- Malocclusion
- Growth asymmetry
- Poor mastication
- Osteomyelitis
- TMJ syndrome
- Salivary disorders
- OSA
- Chronic pain






