
The Case
A kid got his finger caught in a car door. It hurt. The nail is now “all cracked and mangled.” Mom is worried that he’ll never be a hand model. On exam you see the following:

I can see why this freaked mom out
You subsequently get an X-Ray:

Again with the tiny arrows… and yes I realize it isn’t the same finger
The Diagnosis
This patient has a nail-bed laceration in association with a distal phalanx fracture. This is technically an open fracture. Therefore, in addition to repair of the laceration and splinting of the finger, one should also prescribe antibiotics. Distal phalanx fractures are, not surprisingly most often related to crush injuries. A number of structures may be involved, perhaps most (cosmetically) important the nail matrix. It is the subungual tissue from which new nails germinate and migrate. The anatomy is illustrated below:
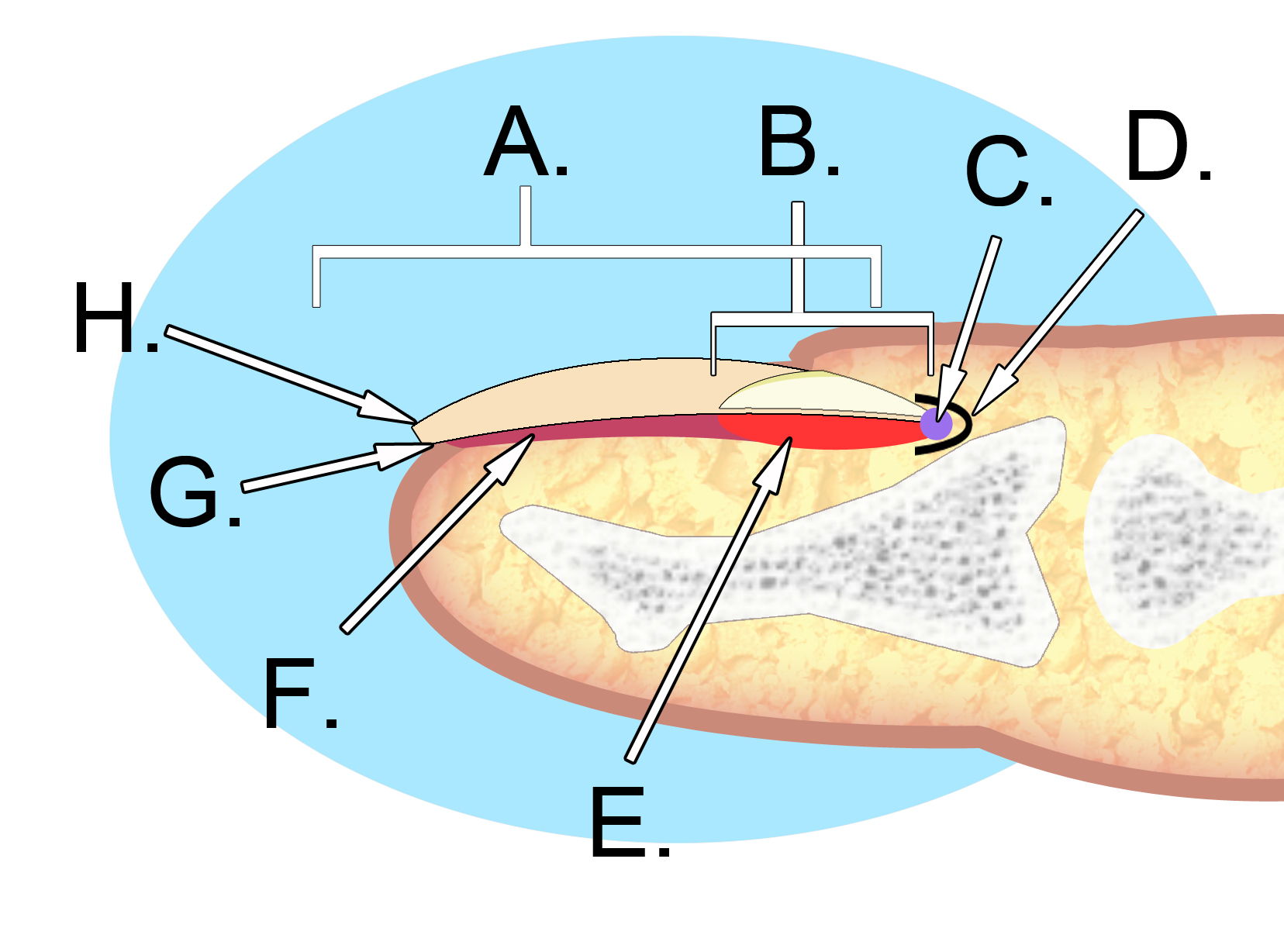
A. Nail plate; B. lunula; C. root; D. sinus; E. matrix; F. nail bed; G. hyponychium; H. free margin
Disruption of the germinal matrix can lead to impaired or no nail regrowth.
Management
The first things that you want to assess for include open injury/major lacerations, neurovascular deficits, rotation, or dislocation, and tendon dysfunction. If the patient can flex and extend at the MCP, DIP and PIP and has good color and sensation then you can be reassured that there are no major neurovascular or tendon/ligament injuries. Simple nondisplaced distal phalanx fractures can be managed by splinting with the DIP in extension for 3-4 weeks. A molded aluminum splint in a U shape can protect the injured digit. A stack splint could also be used. It is not necessary to immobilize the PIP joint.
A fractured distal phalanx with a rotation deformity will need to be reduced. Referral to a hand surgeon is indicated in:
- Fracture + tendon injury
- Fracture + nerve dysfunction (loss of two point discrimination)
- Displaced/angulated transverse fractures
- Intraarticular fractures
- Severe nail bed or nail plate injuries
If there is subungual bleeding this can lead to significant pain. This blood will need to be evacuated in many cases. This figure may help delineate the decision between terphination vs removal of the nail and sutured repair.

Patients with the combination of nailbed laceration and distal phalanx fracture technically have an open fracture. The use of antibiotics is controversial. Stevenson et al performed an RCT and saw no difference in adults treated with prophylactic antibiotics vs not in terms of superficial, deep or bone infections. There is little literature to guide management in kids, and as such I generally prescribe a first generation cepahlosporin (cephalexin) for a week. Clindamycin would be appropriate for penicillin allergic patients.






Great post! Although the Zoolander/David Duchovny hand model reference is WAY better.
https://www.youtube.com/watch?v=EUvgqItrt1c
Have you covered Seymour fractures? http://www.orthobullets.com/hand/6000/seymour-fracture
Couldn’t agree more with the reference! I did post on the (very closely) related extra-octave fracture in the past http://www.pemcincinnati.com/blog/fracture-fridays-cant-put-finger/