
The Case
A 16 year old pitcher presents to the ED complaining of right elbow pain. There is no history of direct trauma, and it has been “hurting more and more over the past few weeks.” He is here because he was told by his coach at practice earlier in the day that he wouldn’t be allowed to pitch in the playoffs tomorrow unless he was seen by a doctor first. On exam his right arm is neurovascularly intact. He has pain along the dorsum of the elbow at the very proximal end of the ulna. The pain is worse when he rests his elbow on the bedside table. You get an X-Ray, because without it this teaching case would be boring.

The elbow X-Ray, with something that looks weird right where your patient hurts
The Diagnosis
This X-Ray shows a fracture of the olecranon. It is not unsurprising that there was no history of trauma, because this can present as a stress fracture. Interestingly there is a high prevalence in children with osteogenesis imperfecta – and this injury has been known to lead to the diagnosis in milder phenotypes. In many cases this injury is the result of traction of the triceps on the olecranon when the arm decelerates at the end of the throwing motion as well as impaction of the olecranon itself into the adjacent fossa. It should be considered along with little leaguer’s elbow as common overuse injuries in young baseball players.
Interpreting X-Rays in the elbow is a topic in and of itself, but suffice it to say knowing the normal anatomic landmarks of the elbow is helpful. I took a picture of a drawing from Netter.

Scanned from god ‘ole Netter
There’s one other thing to mention about X-Rays before we move on. I’m not a big fan of acronyms (especially ones that aren’t really words), but if you are this one may help. It reviews the ossification centers of the elbow. An olecranon that is ossifying could be mistaken for a fracture.
- C- Capitulum, (3 months)
- R- Radial head, (5 years)
- I- Internal (medial) epicondyle, (7 years)
- T- Trochlea, (9 years)
- O- Olecranon, (11 years)
- E- External or Lateral epicondyle, (13 years)
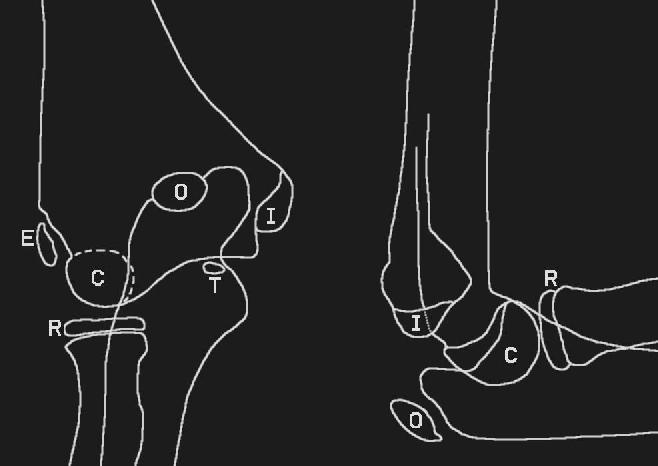
Ossification centers of the elbow in cartoon form
Management
Non-displaced fractures (like the one above) can be managed with rest. So for the young man above, the season is over, as he needs a few weeks of no throwing, followed by gradual return to play. This injury would be appropriate for sports medicine referral as well as ortho. Minimally displaced injuries should be splinted with a long arm posterior splint, and seen by ortho. Fractures with more significant displacement (though exact distance is hard to come by) may benefit form ORIF. See the below image for an example.

The patient from the beginning of the post is happy that this wasn’t his X-Ray





